Abstract
In Saudi Arabia, the use of mobile health (mHealth) applications is one of the modern approaches that had been implemented to enhance the provision of healthcare services in response to the COVID-19 pandemic. This study aimed to explore the perception towards mHealth applications among healthcare professionals. This cross-sectional study recruited 300 health providers using a stratified random sampling technique in a tertiary hospital. A self-administered questionnaire measured demographics, the rate of utilization of applications, and the perception towards its effectiveness for monitoring COVID-19 patients. The results indicate that 84 percent of respondents strongly believed in the role of mHealth apps during the pandemic and 82 percent used them. There was a significantly high perception across male, young, and high- income providers (p <0.05). Many providers agreed that these apps were useful to improve coordination among professionals (52 percent) and reduce travel needs (63.4 percent). Finally, most providers found mHealth apps effective to enhance the quality of patient-centered care.
Key words: COVID-19, Healthcare providers, Mobile health apps, mHealth, Utilization
Introduction
The 2030 vision of Saudi Arabia (Saudi Vision 2030) which provides a roadmap for national economic growth, global engagement, and enhanced quality of life , is encouraging the use of mobile health (mHealth) applications in the healthcare industry to improve healthcare activities. The implementation of new technology in the healthcare system is a significant way to improve healthcare services and outcomes through accessible healthcare.1 mHealth is the practice of using remote communication mobile devices to support electronic healthcare delivery.2 mHealth is now the basis for many effective applications in numerous healthcare fields including disease expectation, prevention, management, diagnostics, treatments plan, and patient education.3
A 2020 study explained that the application allows healthcare consumers to access healthcare from anywhere; it provides the means for virtual consultation with healthcare professionals.Moreover, the mHealth application could be used by patients to book appointments, view lab test results, request medication refills, and print medical reports.4 A study released in the same year highlighted that the quality of healthcare services and overall satisfaction levels can be improved by using mHealth applications. It Also referred to the easy and fast medical care received by the users. mHealth utilization is still low in the kingdom of Saudi Arabia (KSA), due to factors including lack of exposure, awareness, and suitable skills to use the latest cellphones and its continuous updated software systems.5
COVID-19, was first identified in December 2019 in Wuhan.6 In February 2023, the cumulative number of newly diagnosed cases was 828,294, and 69,198,422 vaccination doses so far were taken all over the kingdom. 7
To control the spread of the COVID-19 virus at the beginning of the crisis, the Saudi government adopted emergency actions nationwide, including the closure of schools, universities, workplaces, and quarantine to protect the community.8 The Saudi government has worked to provide smart applications on mobile phones that are designed to provide protection as well as healthcare services for citizens and residents. The ministry of Health approved and implemented multiple mHealth apps as an immediate response to the novel coronavirus in KSA, including: Tawakkalna (indicates the infectious status of the users by colored codes, detects violation of the control procedures and books for vaccination), Tabaud (tackles the spread of COVID infection; helps users to know if they contacted positive people and ensures social and physical distancing), Rest Assured (Tataman) (provides healthcare and assurance for citizens and residents during home isolation or quarantine; preserves their wellbeing and supports their recovery measures), Mawid (helps patients to reserve appointments in primary healthcare facilities in coordination with the concerned specialty), Sehhaty (allows users to access medical information and health e-services including PCR-testing and vaccination which are supplied by various health facilities in the Kingdom), and Seha (provides patients with virtual medical consultation from professionally licensed Ministry of Health (MoH) physicians of different specialties). 9
The importance of mHealth adoption has become more valuable with the spread of the COVID-19 pandemic. At the present time, it is expected that 89 percent of the population uses the internet, and most of the population in Saudi Arabia has access to different types of smart devices such as smartphones, laptop computers, and desktop computers.10 Furthermore, the 2030 vision considered mHealth as a crucial transformational step to reach a high-quality and patient-centric care approach. The MoH’s Sehhaty mobile health app is one example that clarifies how the adoption of mHealth could provide justifiable solutions to improve access and satisfaction with healthcare services. The app provides a complete personal health record and educates patients. The uses of mHealth in Saudi Arabia were efficient in decreasing the cost, time, and amount of effort required to provide care for patients. 11
The use of the mHealth apps by health professionals could enhance the utilization and adoption by patients. These applications could increase care accessibility, improve health outcomes, and satisfaction with the provided services. Therefore, this study aimed to explore the utilization rate and perceptions regarding the effectiveness of mHealth applications among Saudi healthcare providers in response to the COVID-19 pandemic.
Methods
Study design and settings
This descriptive, cross-sectional study was conducted from April to June 2021, at a governmental tertiary healthcare facility in Jeddah, Saudi Arabia. It provides secondary and tertiary healthcare services for more than 76,000 patients throughout the past 6 months and works 24/7 with 43,675 bed capacity.12
Sampling and target population
The target population were healthcare providers actively enrolled in work at the concerned health facility, during the study period. A power analysis using the G*Power calculator was used to verify the required sample size. In G*Power, a multiple regression omnibus (R2 deviation from zero) test was utilized for prior power designs to test whether the eight predictors can be used to explain the healthcare providers’ perceptions towards mHealth applications. The alpha was set at an acceptable level of 0.05, power was set at the level of 80 percent, and the medium effect size was set for this analysis. The test indicates a sample size of 108 was needed.
The study subjects were recruited through a stratified multistage random sampling technique. The hospital included 14 clinical departments, each was including a definite number of health providers (physicians, nurses, and technicians). In the first stage, we randomly chose nine departments to reach the computed sample size. Then we randomly selected a sample from every category of health providers working in the chosen departments considering the inclusion criteria. The sample size has been increased to 300 to represent most of the healthcare professionals in the hospital.
The inclusion criteria included enrollment of active Saudi and non-Saudi healthcare professionals who directly contact patients. The exclusion criteria comprised non-active healthcare professionals (those on vacation), physicians and nursing staff who were in internship year or training scholars, as well as healthcare workers who were in direct contact with patients.
The research received institutional ethical approval from the Research Ethics Committee at Batterjee Medical Colleges (BMC) Jeddah branch, Saudi Arabia with approval reference code number (Res 2021-0003). The survey was conducted in full agreement with the Declaration of Helsinki (2000). Informed consent was highlighted on the front page of the questionnaire. Confidentiality was assured for all participants.
Procedures
The concerned data was collected through an anonymous self-administered questionnaire, which was structured based on a review of similar literature.13,14 The questionnaire consisted of two parts, the first included sociodemographic information, the rate of mHealth applications’ use in medical practice, and the history of COVID-19 infection. The second part measured the degree of perception towards the effectiveness of mHealth applications for monitoring COVID-19 patients through 13 questions followed the Likert scale; responses ranged from 0 (strongly disagree) to 5 (strongly agree). Therefore, the minimum score was 0 and the maximum was 65. The questionnaire took around 4 to 5 minutes to complete. It was structured in the English language and tested for its validity by three experts whose feedback was taken into consideration, and reliability was good (Cronbach Apla was 0.89). Data was collected through interviews with the investigators who used Google Form to gather data from the sampled study subjects.
The investigators were allocated to the previously randomly chosen departments and contacted the selected study subjects who were provided with a QR code for the survey link or received the link via their professional emails. The selected providers filled in the questionnaire anonymously. Once they submitted the form, their responses were saved automatically in the Google Excel spreadsheet ready for data management.
Statistical analysis
The recruited data was exported from the Excel spreadsheets, then tabulated, organized, and analyzed by using the (SPSS) software program version 26. All scores were summed up for each participant and then divided into three categories of self-perception regarding the use of mHealth apps: mHealth believers: ≥44; mHealth opened: 22-44; and mHealth skeptics: ≤ 21.
Descriptive statistics were presented by frequency and percentage for qualitative variables, while mean and SD presented the quantitative variables. Demographics were the explanatory variables, and the outcome variables were the levels of perception towards the effectiveness of mHealth apps, as well as the degree of its utilization. The Chi-squared test was used as the inferential test of significance between substantial groups for selected demographic variables. While the Montecarlo Exact test was used when 25 percent of cells with the observed and expected observation were less than 5. The level of significance was adopted at P <0.05.
Results
This study enrolled 300 healthcare providers. Table (1) showed that 52 percent were females, more than half aged between 26 and 35 years old (58 percent), and of Saudi nationality (54 percent). The greatest proportion of the recruited participants had a master’s degree and were physicians (62.7 percent, and 45.3 percent respectively). Most of the providers had negative medical morbidity (65 percent) while (10 percent) of them reported having hypertension and asthma.
Table 1 also indicated the utilization of the mHealth applications; all the study subjects used governmentally implemented apps including Sehhaty and Tawakkalana, while half of them had Tataman and Mawaid. Few providers sometimes used other applications such as BMJ Best Practice, and Epicorrate in clinical field practice. It was noticed that 8 percent used those apps when they got infected with COVID-19. Regarding the history of COVID-19 infection, the majority of participating providers reported a negative history of infection (92 percent), and only (8 percent) were infected. Whereas smokers represented 20 percent of the overall participants
Table 2 shows that the providers promptly supported the different benefits of mHealth apps, where 48 percent, 52 percent, and 63.4 percent strongly agreed about the efficiency of apps in appointing for the COVID-19 vaccine, overcoming the distance barrier against accessibility to healthcare, and facilitating the coordination between health professionals, respectively .
Table 3 indicates that more male providers strongly believed in mHealth uses (93.6 percent) than females (73.6 percent) (p=0.004). mHealth believers were more significant among younger age groups and single providers; where mHealth believers presented 94 percent of age interval (20 - 25 ) years and 97.2 percent of single providers. Compared to 25 percent among those aged more than 45 years and 78.7 percent of the married providers were mHealth believers.
Discussion
This cross-sectional study analyzed the data of 300 healthcare providers in a tertiary healthcare facility related to the MoH to examine the factors that impacted the utilization of mHealth applications by health professionals in response to the COVID-19 pandemic. The demographic results showed that more than half of the respondents were between 26 to 35 years old (58 percent). Age groups were similar in a study of 2020 who found that younger subjects are more likely to use the mobile application by themselves than older patients. 15
For the utilization of mHealth applications, the result of the question (“Do you have at least one of these applications on your mobile phone?”) revealed that Sehhaty and Tawakkalana apps powered by MoH are the most popular among the participants. That is definitely because Tawakkalana became mandatory by the Saudi government in response to the pandemic, it targets all citizens and residents. The Sehhaty app provides access to medical records that might be used in medical practice. Therefore, the healthcare provider's responses were based on their personal experiences. The second tier of commonly used apps included Tatamman, Mawid, and Tabaud. Participants also reported frequently using other medical applications such as BMJ Best Practice and EpiCorates to support clinical decisions. In general, the results showed that most of the participants (71.3 percent) used at least one of these applications during early the COVID-19 pandemic between January to March 2021 for monitoring and following up on patients, and 28.7 percent of the participants mentioned they never used those mHealth apps.
On the other hand, a recent cross-sectional study in 2021 assessed the utilization of mHealth applications among patients and found that the use of the Sehhaty application made up only 13.1 percent of the recruited patients, which is less than our detected utilization rate.16 That difference could be attributed to the purposeful and oriented use of medical apps between health providers. Meanwhile, our study findings were consistent with a national survey that measured the general population’s use of MoH health applications and revealed a higher utilization rate, which was 47 percent .17.
The present study found no major difference in the perception of mHealth between various professions of healthcare providers. The same observation was detected by a 2019 study, which explained that these technologies have become more commonplace. However, a study reported a difference between different clinical job ranks, where registrars were the highest users of mHealth technology (54 percent) compared to residents (36 percent) and consultants (9.7 percent) .18
Our analyisis indicated a signficant association between believing in mHealth and younger age category , this is could be explained by the authors that the younger generation is more likely to adopt technology than the older ones.
In the literature on understanding gender differences in mHealth adoption, it is stated that males had a higher level of mHealth adoption intention compared with females.19 To make inferences on gender and age, further research is needed as few studies examined the gender effect on using mHealth during the COVID-19 era. The current study revealed that mHealth believers predominantly were male (93.6 percent).This finding contradicts a previous study that reported the utilization of smart device technologies during medical care settings was more frequent among females than males.18 in addition, a 2016 study reported that female physicians more strongly agreed that personal digital devices enhanced their clinical performance.20.
Considering marital status, single health providers accounted for a larger percentage of mHealth believers than married ones, who might have more time and faster rate of work performance. That is in alignment with the above-mentioned observation that younger age is significantly associated with a strong agreement regarding mHealth apps' usefulness. Likewise, having more than enough income was a significant contributor to being mHealth believers since the high income allows the acquisition of advanced technology and a higher-quality network.18 Moreover, the providers in that group might themselves be users of personal wellness/health applications.
The self-perception of the healthcare providers regarding using mHealth apps revealed a high utilization and acceptance rate; (44 percent) of healthcare providers agreed that they would use video conferencing consultation, and half of participants would prefer to use distance consultations for minor health problems, and to monitor treatment of COVID - 19 patients.
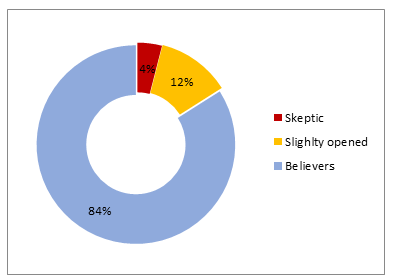
Fig2. Perception of studied healthcare providers regarding the utilization of mHealth apps in monitoring patients during the COVID-19 Pandemic
As shown in Fig. 2, mHealth believers represented 84 percent of all providers, a much higher rate than a related prior report, which declared that 43.3 percent of recruited physicians were strongly confident in eHealth during managing their HIV/AIDS patients.21 This enormous discrepancy could be explained by the fast breakthrough of digital health technology and its prominent deployment during the COVID-19 crisis and its consequences.
Furthermore, the finding of this study detected a significant association between believing in the role of mHealth apps and negative COVID-19 infection history. In alignment with the findings, the number of users who have used mHealth apps is higher than that of those who have not used them. The not infected group with COVID-19 represented 82 percent (n=246) of the total sample, 85.3 percent (n=210) of this group were found to be mHealth believers. That could reflect an indirect relationship between increased utilization of mHealth apps and reduced infection rate of COVID-19 cases in Saudi Arabia during the late phases of the pandemic. For instance, during the COVID-19 pandemic, mHealth apps have been used for tracing and monitoring contagious cases and their contacts.22 Consistently, three apps (Tawakkalna, Tatamman, Tabaud ) were quickly developed and made available within three months of the pandemic emergence. All the different apps served different needs and they were modified to provide sound information about COVID-19 to raise people's awareness.23 Of note, neither educational qualification level nor nationality of the studied providers influenced the perception level regarding mHealth apps’ usefulness.
Moreover, our results showed that most of the healthcare providers believed that the development of mHealth applications can provide some advantages including improving coordination among different health professionals ( 52 percent strongly agreed, 38 percent agreed), reducing travel needs (63.4 percent strongly agreed, 18 percent agreed) , and serving medically deprived areas (36 strongly agreed, 50 percent agreed). A prior study supported similar results, where a big proportion of the recruited physicians agreed that due to the provision of digital health, the clinical decision is facilitated, patient safety is improved, and contact between providers is enhanced. Also, it favored the dissemination of medical skills and experiences between professionals. 21
In line with our findings, a related study highlighted that telemedicine services and patient mHealth applications are valuable tools and viable options for delivering high-quality of care to patients, with less travel and waiting times and lower risk of hospital-acquired infection.22
Another study reported that adopting such applications could address some of the basic issues in the health system, such as limited resources, long waiting times, and general dissatisfaction with health services.16
A 2021 study aimed to explore the effect of using a mHealth application in a telemedicine setting in Abu Dhabi and found that the majority of the mHealth “Remote Care” application users recommended others to use the mobile application for getting healthcare services (79.88 percent). Similarly, 33 percent and 53 percent of the participants in our study strongly agreed and agreed to recommend using current popular mHealth apps to stay updated and informed about the symptoms of COVID-19 disease. 24
Several health applications for managing COVID-19 have been launched and used in Saudi Arabia and globally. Issues such as privacy, safety, security, and data protection remain the major concerns for users.15,25 Current findings show that 36.6 percent strongly agreed and 28.6 percent of providers agreed about the possibility of breaching the privacy and confidentiality of patients’ information while using mHealth apps. That replicates a 2020 study that investigated the attitudes of physicians who treat HIV patients regarding the eHealth. Results found that 80 out of 219 physicians (36.5 percent) strongly opposed the eHealth technology, since it challenges the confidentiality of clinical data and thought out that is a threat for medical information security.21
The present study demonstrated that around half of health providers strongly agreed (45.3 percent) or agreed (50 percent) that mHealth applications are of worthwhile benefit in tracking patients' health data. That was consistent with a related study in the US that assessed healthcare providers' perception regarding specific apps for tracking health status.13 Former literature mentioned that patient-generated health data would facilitate the communication between patients and health professionals, help to define the goals, and identify the patient’s preferences and expectations. Furthermore, when patients receive sufficient information, better health outcomes would be achieved.26,27
This could be contributed to the providers’ beliefs that patient-generated data are more trustworthy and reliable than the patient's self-report, that sometimes mispresents his/her medical status, and to avoid the recall bias of the patient's medical history.
In addition, our research has demonstrated that 50 percent of healthcare providers prefer to use distance consultation to monitor the compliance to treatment between the COVID-19 patients. Consistently, it was reported that mHealth applications is one of the significant methods to assure adherence to medications uptake.28,29
Likewise, the current study demonstrated that 48 percent of providers strongly agreed with using the apps to make appointments for vaccinations against COVID-19 infection, to facilitate high administration of the vaccines.
Previous studies have concluded that mHealth applications were useful to enhance appointment procedures among patients of various clinical issues. For instance, it facilitated healthcare provision for HIV–positive pregnant females, reminding women for routine postnatal care, fostering childhood immunization coverage, and ensuring adherence to the periodic follow up for patients with non-communicable diseases.29-32
Overall, the study findings reflected an advent of mHealth applications between the studied providers due to the transformative effect of this technology on healthcare delivery, particularly for health monitoring and management, where 24 percent strongly agreed and 44 percent agreed that mHealth technology will speed progress toward more individualized diagnosis and treatment. Similar literature pointed out its significant role in this regard. 33,34
Conclusion
Findings revealed a high rate of mHealth believers among the studied providers who showed significant variations across their age, gender, social status, and level of income in terms of self-perception regarding effectiveness of mHealth. Many professionals perceived that mHealth apps were useful for providing remote counseling. Most providers recommended utilization of health information technology for checking and monitoring on COVID–19 patients. That would positively imply medical practice. Further research should be conducted to study this area in focus and on a wider scale, as mHealth and eHealth are rapidly growing sectors of health transformation in the kingdom.
Study Limitations
There are several limitations. First, the cross-sectional design of the study didn’t allow for casual relationship analysis. Second, the data was collected through a questionnaire which was structured by the authors according to the prevailing pandemic circumstances. We didn’t deploy one of the standard technologies adopting models due to their simplicity and narrow spectrum which focuses on general individual’s perceptions towards usage of technology. That rendered those models inappropriate to our study’s aim and target population. Third, the data regarding the adoption and utilization of mHealth were self-reported and might be overestimated.
References
1. Ren J.,Liu C., Gao Q., Yang L., Huang X., Guo Q. Use of appropriate healthcare technologies: A cross-sectional study in rural Zhejiang of China. BMC Health Serv Res. (2015); 15:295.
2. Iyengar S.R. Fundamentals of Telemedicine and Telehealth.eds: Gogia SH Mobile health (mHealth). Academic Press. (2020); Ch12: 277-294. ISBN 978-0-12-814309-4. https://doi.org/10.1016/B978-0-12-814309-4.00012-4.
3. Alanzi T. A Review of Mobile Applications Available in the App and Google Play Stores Used During the COVID-19 Outbreak. J Multidiscip Healthc. (2021); 12 (no.14):45-57. DOI: 10.2147/JMDH.S285014. PMID: 33469298; PMCID: PMC7812813.
4. Agarwal N. and Biswas B. Doctor consultation through mobile applications in India: An overview, challenges and the way forward. Healthc Inform Res (2020); 26:153-8.
5. Jadi Amr. Mobile Health Services in Saudi Arabia-Challenges and Opportunities. International Journal of Advanced Computer Science and Applications. (2020); 11. DOI: 10.14569/IJACSA.2020.0110422.
6. Center for Disease Control and Prevention (CDC). Basics of COVID -19.. Access on June 2023.
7. Saudi Ministry of Health (MOH)a. Prevalence of problem at the national level. Accessed on February 8, 2023.
8. mHealth application used in KSA, available at: https://www.moh.gov.sa/en/Support/Pages/MobileApp.aspx. Accessed February 5, 2021.
9. Saudi Ministry of Health (MOH). Accessed on April 4, 2021.
10. Otaibi M.N. Internet of Things (IoT) Saudi Arabia Healthcare Systems: State-Of-The-Art, Future Opportunities and Open Challenges. Journal of Health Informatics in Developing Countries. (2019).
11. Hassounah M., Raheel H., Alhefzi M. Digital Response During the COVID-19 Pandemic in Saudi Arabia. J Med Internet Res. (2020);22(no.9): e19338. DOI: 10.2196/19338.
12. Ministry of Health (MOH). King Abdullah Medical Complex-Jeddah: 76+ Thousand Patients Served in 6 Months, March 2018 access on 23 Jan (2021). available at: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/news-2018-03-06-005.aspx
13. Holtz B., Vasold K., Cotten S., Mackert M., Zhang M. Health Care Provider Perceptions of Consumer-Grade Devices and Apps for Tracking Health: A Pilot Study. JMIR Mhealth Uhealth. (2019);7(no.1): e9929. DOI: 10.2196/mhealth.9929. PMID: 30668515; PMCID: PMC6362391.
14. Kong T., Scott M.M., Li Y., Wichelman C. Physician attitudes towards-and adoption of-mobile health. Digit Health. (2020); 6:2055207620907187. Published 2020. doi:10.1177/205520762090718.
15. Istepanian R.S., and AlAnzi T.U., Chapter Twenty Two - Mobile health (m-health): Evidence-based progress or scientific retrogression, In Biomedical Engineering, Biomedical Information Technology (Second Edition), (2020), Pages 717-733, ISBN 9780128160343, https://doi.org/10.1016/B978-0-12-816034-3.00022-5.
16. Alharbi R., Qadri A., Mahnashi M., Hakami A., Darraj B., Shnaimer J., Gosadi I. Utilization of Health Applications Among Patients Diagnosed with Chronic Diseases in Jazan, Saudi Arabia During the COVID-19 Pandemic. Patient Prefer Adherence. (2021); 15:2063-2070. https://doi.org/10.2147/PPA.S329891.
17. Alharbi A., Alzuwaed J., and Qasem H. Evaluation of e-health (Seha) application: a cross-sectional study in Saudi Arabia. BMC Med Inform Decis Mak. (2021); 21: 103.